
Episode 064: Does Cannabis Use Increase Schizophrenia and Psychosis?
No Psychiatry CME credits for this episode.
Other Places to listen: iTunes, Spotify
Article Authors: Victoria Agee, BS, David Puder, MD
There are no conflicts of interest for this episode.
Background: Cannabis, Psychosis and Schizophrenia: Unravelling A Complex Interaction
(Andreasson, 2015) (Hamilton, 2017)
1970’s was when researchers first started looking into cannabis as a cause of psychosis. Scientists began asking if cannabis could be responsible for a short-term psychotic reaction or if it was a trigger for longer-lasting schizophrenia.
In the 1980’s, Sven Andreasson looked at Swedish population where cannabis was fairly pervasive. He used a military conscript registry of 45,570 swedish men and found that 4,290 (9.4%) of the conscripts had used cannabis at least once. (7% chose not to answer which could have significantly changed the study.) Andreasson described frequent use of cannabis as 50 or more occasions and infrequent as less than that. He was able to show a dose-response relationship between cannabis and schizophrenia. Importantly, of the 274 conscripts who had a diagnosis of schizophrenia at follow-up, only 21 were frequent cannabis users. This lead to the idea that cannabis use might be caused by an emerging schizophrenia: schizophrenia precedes cannabis use.
Important to note that schizophrenia can lie dormant until a person is exposed to a trigger, such as a psychoactive drug. This leads to the idea that cannabis could have triggered schizophrenia in a small vulnerable population within their sample.
Andreasson himself said “A statistical association between cannabis and schizophrenia does not imply causation. Cannabis consumption might, on the contrary, be caused by an emerging schizophrenia”
Further studies were done in the 1990’s. However, it was difficult to compare study groups as there is no consistency in how cannabis consumption and potency had been measured. It was also during this time that the DSM and ICD recognized cannabis psychosis as a distinct diagnostic category.
1998, Wayne Hall did a review focused on the two dominant hypotheses: heavy cannabis causes a specific cannabis psychosis and cannabis use precipitates schizophrenia and made the symptoms worse. However, found a lack of controlled studies. There were often compounding bias. Additionally, finding a person with schizophrenia who solely used cannabis was rare as most would most likely have also used alcohol, which in and of itself has psychogenic properties.
Serious Psychological Distress (SPD) and Daily Cannabis Use, 2008 to 2016: Potential Implications For Mental Health?
Approximately 25% of cannabis users in the US use every day or nearly every day, which is a significant increase in the last 10 years
As the number of cannabis users increases and it continues to be legalized, it is important to show what groups are at greatest risk to have negative consequences
In April 2019, a study published that looked at the prevalence of cannabis use in people who did and did not have “serious psychological distress, ” which is defined as feelings of worthlessness, hopelessness, sadness, and/or nervousness.
In 2008, the prevalence of cannabis use among persons with SPD was nearly 2.5 times that among persons without SPD. From 2008 to 2016, the prevalence of daily cannabis use in persons with SPD increased from 3.89 to 8.07. There was also an increase in prevalence in daily cannabis use across nearly all demographic subgroups. In 2016, persons with past-month SPD were more than twice as likely to report daily cannabis use compared to persons without SPD (OR = 2.38, 95% CI = 1.89, 3.01).

Prevalence of daily cannabis use for those with and without serious psychological distress (SPD) from 2008 to 2016.
Association Of Cannabis Use in Adolescence and Risk of Depression, Anxiety, and Suicidality in Young Adulthood: A Systematic Review and Meta-analysis. (Gobbi, 2019)
In a meta analysis that covered 11 studies comprising 23 317 individuals, the odds ratio of developing depression for cannabis users in young adulthood compared with nonusers was statistically significant 1.37, for suicidal ideation was 1.50, and for suicide attempt was suicidal attempt was 3.46.

Forest Plot Showing Adjusted Odds Ratio (OR) and 95% CIs for Depression and Anxiety in Young Adulthood According to Cannabis Use in Individual Studies
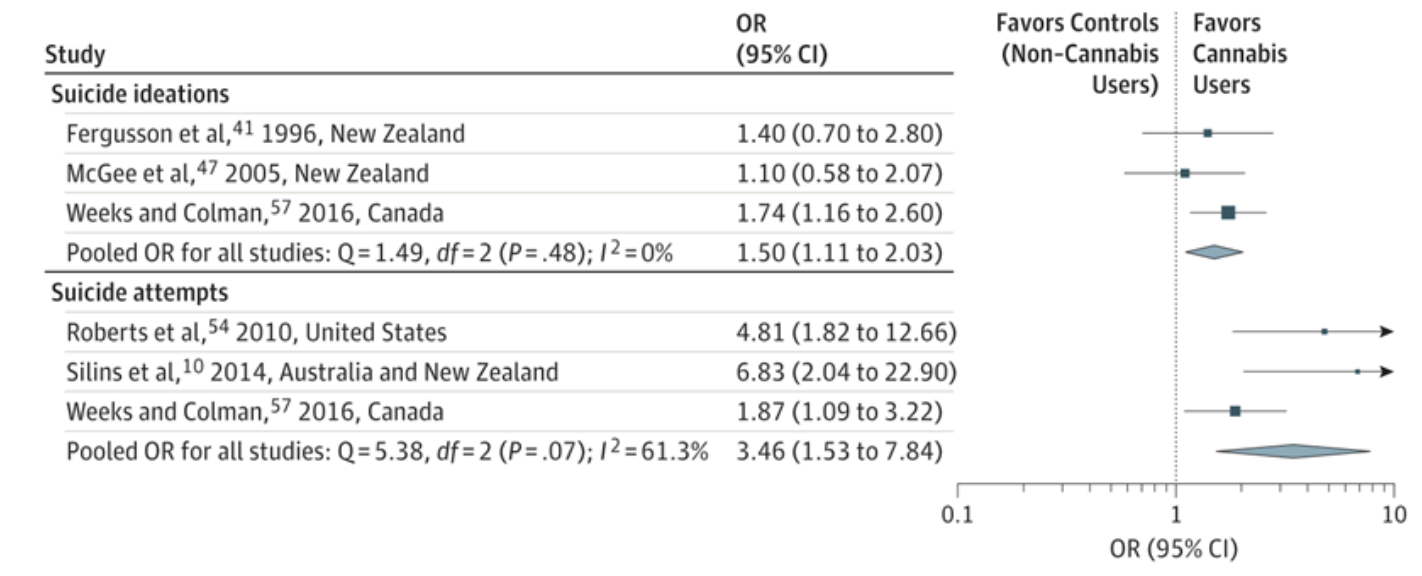
Forest Plot Showing Adjusted Odds Ratio (OR) and 95% CIs for Suicidal Ideations and Attempts According to Cannabis Use in Individual Studies
Leads Back To The Two Hypotheses:
Individuals with SPD use cannabis for its negative reinforcement effects, e.g., to reduce or remove distress-related symptoms, anxiety, or stress
While cannabis use might ameliorate immediate symptoms of stress or distress, it might contribute to longer term persistence of symptoms.

Picture Credit: Tori Burghart
Cannabis Increases Risk of Psychosis
The contribution of cannabis use to variation in the incidence of psychotic disorder across Europe(EU-GEI): a multicentre case-control study. (Di Forti, 2019)
Study of 11 sites across Europe and Brazil. 901 patients with first-episode psychosis across 11 sites and 1237 population controls from those same sites. Looked at potency and its relation to psychotic symptoms. High potency >10% THC and Low potency <10%. To determine the potency, Participants were asked to name, in their own language, the name of the type of cannabis they mostly used during their period of use. Those strains were then compared with national potency data compiled by various other studies. (See Di Forti Supplemental Material)
Patient selection: Patients presenting with their first episode of psychosis were identified by trained researchers. Patients were excluded if they had been previously treated for psychosis, met criteria for organic psychosis (some pathological effect on the brain), or had acute intoxication psychosis. Compared with controls, cases were younger, more often men, and from ethnic minorities.
Daily cannabis use was associated with increased odds of psychotic disorder compared with never users (adjusted odds ratio [OR] 3.2, 95% CI 2.2–4.1), increasing to nearly five-times increased odds for daily use of high-potency types of cannabis (4.8, 2.5–6.3). The population attributable fractions calculated indicated that if high-potency cannabis were no longer available, 12.2% (95% CI 3·0–16·1) of cases of first-episode psychosis could be prevented across the 11 sites, rising to 30.3% (15.2–40.0) in London and 50.3% (27.4–66.0) in Amsterdam. This is most likely due to the high rate of daily cannabis use in those cities. There was a positive correlation between the incidence rates for psychotic disorder and prevalence of high-potency cannabis use (r=0.7, p=0.0286) and daily use ( r=0.8, p=0.0109).

Fully adjusted ORs of psychotic disorders for the combined measure of frequency plus type of cannabis use in three sites
Data are shown for the three sites with the greatest consumption of cannabis: London (201 cases, 230 controls), Amsterdam (96 cases, 101 controls), and Paris (54 cases, 100 controls). Error bars represent 95% CIs. OR=odds ratio.

Adjusted incidence rates for all psychosis for the 11 sites plotted against the prevalence of daily use in the population controls (A) and prevalence of use of high-potency cannabis in the population controls (B)
Incidence rates are adjusted for age, gender, and ethnicity. Puy-de-Dôme is not included because data on ethnicity were missing for 27 (66%) of 42 incidence cases, therefore the adjusted incidence rate for this site was not calculated.

Crude and fully adjusted ORs of psychotic disorders for the combined measure of frequency plus type of cannabis use in the whole sample
Crude ORs are adjusted only for age, gender and ethnicity and fully adjusted ORs are additionally adjusted for level of education, employment status, and use of tobacco, stimulants, ketamine, legal highs, and hallucinogenics. Error bars represent 95% CIs. OR=odds ratio.
The odds of psychotic disorder among daily cannabis users were 3.2 (CI 2.2-4.1) times higher than for never users. Risk of psychosis with lifetime use of cannabis for low potency cannabis and high potency were 1.1 (CI 0.9-1.5) and 1.6 (1.2-2.2) respectively. Daily use of high potency cannabis was associated with OR 4.78 (CI 2.5-6.3). Those who had started using high-potency cannabis by 15 years old had a 2.3x higher risk of developing psychosis (2.3, CI 1.4-3.1).
Consistent with previous epidemiological and experimental evidence suggesting that the use of cannabis with a high concentration of THC has more harmful effects on mental health than the use of weaker forms.
Responses:
Gillespie stated that the harmful effects of high-potency cannabis use on mental health was likely overestimated due to a lack of adjustment for confounding from genetic and environmental effects. Gillespie performed a meta-analysis that resulted in a statistically significant genetic correlation between schizophrenia risk and risk factors for cannabis use. However, they did not account for cannabis frequency or potency. (Gillespie et. all, 2019)
Other environmental confounding factors such as the air pollution in Europe, specifically nitrous oxide, has been shown to increase risk of psychosis. (Linnman, 2019)
There was no test of the purity of the cannabis that was used. Also, previous studies have shown that most people who have Substance Use Disorder rarely use only one substance. Simply the diagnosis of SUD increased the likelihood of schizophrenia in life, with alcohol and cannabis both contributing. One of the main complaints was that the main researchers (Di Forti et al.) improperly simplified the possible causes of psychosis. (Clark, 2019)
Rebuttal: (Di Forti et al., 2019)
Evidence that shows that removing high-potency cannabis use could prevent up to 50% of new cases of psychotic disorders in Amsterdam, thus inferring that a sizeable proportion of incident cases is caused by cannabis use.
They pointed out that yes, pollution and tobacco can have an effect on psychosis. However, that statement alone does not explain why in cities with less pollution, the incidence rate was lower. There was an effect of tobacco driving the OR, but this was driven in part by cities in Spain and Italy where smoking was more prevalent, both in cases and controls. Proportions of smokers in Madrid, Spain and Bologna, Italy were double that of Amsterdam and in London.
It is unlikely that the types of high-potency cannabis available across the European sites were contaminated by the same pesticides or had the same concentration of metals. As for the polysubstance use, the analysis controlled for the potential confounding effects of other drugs.
As psychosis is a multifactorial disorder, it is important to not negate nor minimize the potential for a genetic factor.
Further support of the link: Meta-analysis of the Association Between the Level of Cannabis Use and Risk of Psychosis. (Marconi, 2016)
A meta-analysis of 18 studies including 66 816 individuals gave an OR of 3.90 (95% CI 2.84 to 5.34) for the risk of schizophrenia and other psychosis-related outcomes among the heaviest cannabis users compared to nonusers.
Assessment of cannabis use with a dose criterion (frequency/amount used/severity) before the onset of psychosis was part of their inclusion criteria. Exclusion criteria included enrolment of subjects known as suffering from mental illness before the use of cannabis or ultra-high risk subjects and. studies examining the comorbidity between substance use disorders and psychosis.

Forest plots including subgroup analyses of the odds ratio of psychosis in the most severe cannabis users. (A) Divided by study design (cohort and cross-sectional). (B) Divided by outcome measure (diagnosis of psychotic disorder and presence of psychotic symptoms).

Estimated risk ratio of psychosis by level of cannabis use in original studies.
Genetic Vulnerability To Psychosis
Baseline heredity in Schizophrenia (Schizophrenia Heredity and Genetics)

Studies Showing How Genes Can Increase Risk of Cannabis Causing Psychosis
GENE-ENVIRONMENT INTERACTION BETWEEN AN ENDOCANNABINOID SYSTEM GENETIC POLYMORPHISM AND CANNABIS USE IN FIRST EPISODE OF PSYCHOSIS. (BIOCHE, 2019)
Looked at 15 specific SNPs of the endocannabinoid system and their interaction with cannabis. Found that FAAH fatty-acid amide hydrolase) rs2295633SNP polymorphism in ligands is associated with increased risk of first episode psychosis in patients with frequent cannabis use but not subjects without a history of cannabis use. It was also found that patients with the homozygous dominant genotype is more likely to present with first episode psychosis (OR 10.69, statistical power 0.78)
COMT VAL 158 MET GENOTYPE AND CANNABIS USE IN PEOPLE WITH AN AT RISK MENTAL STATE FOR PSYCHOSIS: EXPLORING GENE X ENVIRONMENT INTERACTIONS (NEIMAN, 2016)
COMT enzyme plays a crucial role in modulating dopamine levels in cortical and limbic regions of the brain. Individuals with Val/Val genotype have 40% higher COMT enzyme activity in the brain and subsequently lower dopamine levels in the prefrontal cortex. This dopamine dysregulation predisposes a patient to schizophrenia. Hypodopaminergic prefrontal activity, which is closely related to blunted reward processing and cognitive decline has been widely observed in subjects at risk of psychosis and might explain the high levels of comorbidity between cannabis abuse or dependence and schizophrenia spectrum disorders.
Study of 201 patients, 39 patients were homozygous and used cannabis weekly. Patients were assessed with CAARMS, a semi-structured interview used to assess for risk of first psychotic episode. Patients with Val/Val genotype had a statistically significant higher CAARMS positive total score with (t=3.08, p=0.004). Patients with Met/Met genotype had no increased risk of psychosis.
INTERACTIONS BETWEEN VARIATION IN CANDIDATE GENES AND ENVIRONMENTAL FACTORS IN THE ETIOLOGY OF SCHIZOPHRENIA AND BIPOLAR DISORDER: A SYSTEMATIC REVIEW (MISIAK, 2017)
AKT1 (protein kinase 1) rs2494732 CC homozygotes with a history of cannabis use showed a greater than two fold increase in the likelihood of having a psychotic disorder in comparison with the AKT1rs2494732 TT homozygotes.
Among daily cannabis users, individuals with the AKT1 rs2494732 CC genotype demonstrated a sevenfold increase in the odds of developing psychosis compared to the AKT1rs2494732 TT homozygotes.
In female schizophrenia patients, cannabis use was associated with earlier age of psychosis onset in the BDNF 66Met allele carriers, but not in the BDNF66Val/Val homozygotes.
So far, genetic orientated research has failed to provide a plausible explanation involving a purely biological or genetic factor that makes clear the direction of the relationship between cannabis and schizophrenia. Although it is possible that there is a relationship and even if that were to emerge as causal, it would be influenced significantly by the individual’s environment. (Hamilton, 2019)
EXAMINING THE INDEPENDENT AND JOINT EFFECTS OF MOLECULAR GENETIC LIABILITY AND ENVIRONMENTAL EXPOSURES IN SCHIZOPHRENIA: RESULTS FROM THE EUGEI STUDY. (GULOKSUZ, 2019)
The study consisted of 1699 patients and 1,542 unrelated controls. It looked at many of the main environmental factors that had been previously linked with schizophrenia: bullying before age of 16, emotional abuse, physical abuse, sexual abuse, emotional neglect, physical neglect, winter birth, hearing impairment, and cannabis use. All patients were genotyped and given a polygenic risk score for schizophrenia (PRS-SCZ). The published paper (see above link) goes into more detail about how it was calculated.
All individual environmental factors, apart from winter birth, had a statistically significant risk of psychosis.
There was evidence for additive interaction between PRS‐SCZ75 (Schizophrenia risk state with 75% of the risk factors or greater in the genes) and regular cannabis use (RERI=5.60; 95% CI: 0.88‐10.33; p=0.020), childhood bullying (RERI=2.76; 95% CI: 0.29‐5.23; p=0.028), emotional abuse (RERI=5.52; 95% CI: 2.29‐8.75; p<0.001), sexual abuse (RERI=7.61; 95% CI: 2.05‐13.17; p=0.007), and emotional neglect (RERI=2.46; 95% CI: 0.98‐3.94; p=0.001), respectively.

Additive effects of cannabis use, emotional abuse, sexual abuse, emotional neglect and bullying on the association between the polygenic risk score for schizophrenia, 75% cut‐point (PRS) and case‐control status, adjusted for sex, age and ten principal components; RERI – relative excess risk due to interaction.

Conclusion: Positive additive interaction between genetic liability and environmental exposure indicates synergy between gene and environment; that is, the combined influence of genetic liability and environmental exposure is larger than the sum of individual effects of each.
Studies Looking At The Link Between Cannabis Contaminants Playing A Toxic Role
CANNABIS CONTAMINANTS: SOURCES, DISTRIBUTION, HUMAN TOXICITY AND PHARMACOLOGIC EFFECTS (DRYBURGH, 2018)
Unfortunately, there are very few studies on the subject of cannabis contamination.
3 ways of heavy metal introduction into cannabis plant: through absorption in the soil, processing, post-production (heavy metals are added to increase the weight and increase street value)
95 cases of lead poisoning due to contamination of illegal preparations to increase the weight
Case reports of possible arsenic contamination related to cannabis arteritis
Current Therapeutic Cannabis Controversies and Clinical Trial Design Issues (Russo, 2016)
Both American Herbal Products Association and American Herbal Pharmacopoeia have developed guidelines for cultivation and production. However, cannabis is regulated differently state by state.
In California, for medical marijuana, they test samples for pesticides, heavy metals etc. However, not everyone can obtain marijuana legally.
PESTICIDES IN CANNABIS
In a study of 26 samples of legalized cannabis products from Washington, 84.6% of the products contained significant quantities of pesticides including insecticides, fungicides, miticides, and herbicides.
Fifty-seven concentrate samples were screened for cannabinoid content and the presence of residual solvents or pesticides. Considerable residual solvent and pesticide contamination were found in these concentrates. Over 80% of the concentrate samples were contaminated in some form. 8 different pesticides were found in 33% of the samples, most common being paclobutrazol, a pesticide that is not registered with the Environmental Protection Agency (EPA) for use on food crops. Other pesticides were bifenthrin and myclobutanil (Raber, 2015)
Pesticides have shown some negative reproductive side effects, along with GI disturbances. No psychosis has been reported with these pesticides.
As for side effects in humans due to heavy metal/pesticide contamination, we could not find good studies. If you have any, please send them to us.
Psychotic patients use cannabis to combat their symptoms - reverse causation
Although plausible, it should be stressed that several studies show how this is not the main reason these individuals consistently give as their motivation to use cannabis. Pleasure and recreation are the main reasons given by patients.
Evidence of a temporal relationship, with cannabis use preceding the onset of psychosis, has been credibly demonstrated in a number of studies, which argues against the reverse causality hypothesis (Moore et al., 2007)
Studies suggest suggested that those who are vulnerable to developing psychosis might also be more likely to start using cannabis, which in turn may increase the likelihood of their developing a psychotic disorder subsequently. (McGrath et al., 2010)
Conclusion:
We conclude that Cannabis use increases risk for psychosis; especially with use of high potency Cannabis and younger age at the time of use.
There are genes that increase the risk of psychosis with Cannabis use.
Evidence supporting pesticides and heavy metals being the main cause don’t have strong enough evidence but further studies are needed.