
Episode 075: Cancer: Depression, Anxiety, And Hypoactive Delirium–A Dive Into Psycho-Oncology
In this week’s episode we sat down with four guests (detailed below) and discussed different aspects of mental health in humans bravely facing cancer. The below notes go beyond the podcast episode in content and depth and hopefully equips you to have more empathy, compassion and knowledge.
By listening to this episode, you can earn 1 Psychiatry CME Credits.
Other Places to listen: iTunes, Spotify
Article Authors: Shawna Chan, Mona Mojtahedzadeh, MD, Salman Otoukesh, MD, David Puder, MD
There are no conflicts of interest for this episode.
Dr. Mona Mojtahedzadeh’s medical career began in Iran, where her passion for public health and service led her to care for refugee patients and mothers and children impacted by HIV. She completed her psychiatry training, including a fellowship in Consultation-Liaison Psychiatry, in the United States, and she is currently a psychiatrist in the Supportive Care Medicine division at City of Hope.
Dr. Salmon Otoukesh began his medical training in Iran and has extensive experience working with international organizations, such as the United Nations. He completed his Internal Medicine residency and Hematology/Medical Oncology fellowship in the United States, and he specializes in Hematopoietic Cell Transplantation at City of Hope.
Shawna Chan is a 4th year medical student at UC Irvine School of Medicine applying to the Psychiatry residency. She hopes to provide empathetic, compassionate care for those living with cancer, and she is interested in psycho-oncology, pain management, and palliative care.
David Puder is the host of the Psychiatry and Psychotherapy Podcast and is the medical director of a day treatment program “MEND” which treats people with cancer or other medical issues who are struggling with significant depression, anxiety, and other psychiatric issues.
Mental Health In Cancer
Nuances of diagnosing depression: normal cancer symptoms that can be confused with depression are somatic symptoms such as anorexia, sleep disturbance and fatigue.
“Inclusive approach”: count any of MDD criterion, regardless of whether due to medical or psychological cause, although this may result in falsely elevated rates of depression
“Exclusive approach”: excludes anorexia and fatigue, reduced sensitivity
“Substitutive approach”: excludes somatic symptoms related to somatic illness (fatigue, weight loss, psychomotor changes, impaired concentration) and replaces with cognitive-affective symptoms (irritability, tearfulness, feeling punished, social withdrawal)
Each diagnostic scheme comes with its own set of advantages or disadvantages. Ultimately we must rely on clinical judgement—for example, symptoms that are fixed and nonreactive to environmental factors can help distinguish depression from normal grief (Koenig et al, 1997)
Clinical Pearl: Anhedonia and the inability to enjoy one’s life outside the context of cancer is an important feature in distinguishing depression from adjustment disorder or normal grief.
Adjustment disorder: the most common psychiatric diagnosis made in cancer patients
Meta-analysis of heme/onc patients: 19.4% adjustment disorder, 14.9% major depression, 10.3% anxiety disorder (Mitchell et al, 2011)
Psychotherapeutic interventions 1st line, limited research on pharmacotherapy but can temporarily use hypnotics, benzos, antidepressants, etc., to target symptoms
Depressive disorders: ~16% cancer of patients experienced MDD; if including dysthymia and minor depression, occurs in 22% patients
Substance/medication-induced depressive disorder following corticosteroids, exogenous cytokines (IFNa, IL-2)
Differential:
Demoralization: affects 13-18% of cancer patients. Presents as hopelessness, helplessness, loss of meaning and purpose to life. (Robinson et al, 2015)
Hypoactive delirium mimics depression in the medically ill as patients may appear apathetic or have SI. Look for disturbances in consciousness, attention, cognition, and perception.
More often in palliative care setting, older vs. younger patients
Generally due to hypoxia, metabolic disturbances, and hepatic encephalopathies. Other etiologies more specific to cancer population include: brain tumor, leptomeningeal disease, paraneoplastic syndrome, cerebral edema after brain radiation, hypercalcemia, hyperviscosity syndrome (lymphoma, waldenstrom macroglobulinemia).
May be less responsive to pharmacotherapy; also associated with higher risk of mortality
Degree of cognitive impairment much more pronounced in delirium than depression. There is also disturbance in level of arousal
Poorly organized, abrupt onset delusions; predominantly visual/tactile rather than auditory hallucinations
Clinical Pearl: Consider drug-drug interactions if you suspect hypoactive delirium. Anticholinergic medications (e.g. Benadryl), steroids, and benzodiazepines are common culprits. Concurrent use of CYP2D6 inhibitors (paroxetine, fluoxetine for example) with TCAs can increase serum level of TCAs (which are anticholinergic) and lead to hypoactive delirium.
Hyperactive delirium: agitated, restlessness, hypervigilance, hallucinations/delusions; more easily recognized and referred to psychiatrists
Correlated with alcohol/drug withdrawal, intoxication, medications adverse effects
Pharmacotherapy for Depression
Elements that impact medication choice include: prior response history, medical comorbidities, drug interactions, route of administration, onset of action with regards to patient prognosis, other somatic/physical symptoms such as pain, insomnia, hot flashes
SSRIs and SNRIs 1st line for tolerability and safety; SNRIs also help with hot flashes
Bupropion: may improve sexual function and fatigue
Mirtazapine: cancer-related anorexia, cachexia, nausea/vomiting; rare side effect of reversible neutropenia
Trazodone < 100 mg QHS: orthostatic hypotension and dizziness in elderly/fragile
Reboxetine: NRI reported to be effective for apathy, fatigue, concentration, anxiety; activating, so be cautious in comorbid cardiac disease
Agomelatine: novel melatonergic antidepressant that acts on 5-HT2C, sleep promoting, weight natural, lacks sexual side effects and DC effects; LFT monitoring required
TCAs: seldom 1st line due to side effects, but may be used for comorbid neuropathic pain at lower doses than used for depression
Psychostimulants: rapid onset for energizing effects in depressed patients w/ advanced/terminal disease, but unclear efficacy in alleviating depression; prolonged use rarely associated with psychosis, also take caution with cardiac comorbidities
Medication adverse effects: osteoporosis, GI hemorrhage, hyponatremia, serotonin toxicity w/ fentanyl, tramadol, ondansetron, metoclopramide
Psychotherapy: CBT, relaxation strategies, problem-solving approaches in recently diagnosed; existential, life narrative, dignity conserving, meaning-centered interventions in advanced/terminally ill
Suicide: patients w/ cancer are at increased risk for suicidal thoughts and behavior compared with general population and other medically ill; 2x risk of suicide vs. general population
Fleeting wish to die are often normal in cancer patients, although persistent SI, plan, intent are of great concern.
“Wish to hasten death” is a reaction to suffering in the context of a life threatening condition, from which a patient finds no way out other than accelerating death. (Balaguer et al, 2016)
Multifaceted, complex, elements of psychosocial, psychological, neurobiological factors, hence suicide risk assessment is crucial
Clinical Pearl: Suicide assessment in this patient population requires a highly individualized approach and differs from patient to patient. Suicidality in a cancer patient who also suffers from clinical depression is highly concerning and must be appropriately addressed.
Anxiety: 10-30% prevalence in cancer patients, where most often patients report exacerbation of existing problem w/ anxiety due to medical stressor; symptoms persist and remain concern for long-term cancer survivors
Primary challenge is to find underlying causes for anxiety
Steroids and anti-emetics (prochlorperazine) can cause anxiety
Prochlorperazine and metoclopramide are dopamine blockers which can cause akathisia (Weiden, 1985)
Medical conditions - CHF, pleural effusion, PE - also present with breathlessness, chest tightness, palpitations
Clinical Pearl: Dopamine blockers may cause akathisia, characterized by inner feelings of restlessness that mimics anxiety.
Pharmacotherapy: benzos short-term, SSRIs/SNRIs long-term
Benzos: alprazolam, diazepam, and lorazepam have the greatest risk for abuse. Lorazepam, oxazepam, and temazepam (remember “LOT for Liver”) are preferable in liver disease because they are not subject to Phase 1 metabolism. Clonazepam has less abuse liability than shorter-onset agents
Can use other meds that target symptoms - mirtazapine (some evidence, atypical antipsychotics in patients w/ dementia or at risk for delirium (no clinical trials for APDs)
Psychotherapy: educational, CBT, supportive therapy, complementary approaches (acupuncture, massage, creative art therapy, although data mostly from non-blinded studies)
Cognitive-behavioral interventions have greatest evidence
CBT, systematic desensitization, stress management and relaxation (Hermann et al, 2013)
PTSD: difficult to estimate prevalence, but estimated to be 10-20% which is about twice that of the general population; however, full blown PTSD occurs in 5% of cancer patients that must involve sudden or catastrophic events. (Abbey et al, 2015)
Cancer experience is a unique type of trauma that doesn’t entirely remain in the past. Rather, it is ongoing threat that requires participation in clinical encounters that may reinforce the significance of the threat of cancer
Previous trauma increases risk - cancer may not just be independent trauma, but also trigger for existing/dormant traumatic responses
Pharmacotherapy: often antidepressant, can add atypical antipsychotic
Benzos can help with nausea and PTSD
Clonidine and prazosin for nightmares but may be contraindicated with some cancer regimens
Psychotherapy: mainstay of treatment in PTSD, most research looks at patients no longer undergoing active cancer treatment
CBT effective in cancer setting: psychoeducation about distress and PTSD after cancer, breathing and relaxation training, imaginal and in vivo exposure to cancer-related cues, cognitive restructuring, behavioral activity scheduling—benefits may persist despite re-traumatization
“Multimodal approach” is recommended by NCI; evidence best for CBT
Fatigue: in 40% of cancer survivors, 100% of those undergoing active treatment, (Jones et al, 2016). Cancer patients perceive fatigue as more distressing than pain, nausea, or vomiting. Associated with decreased QOL, significant psychological and functional morbidity. Possibly due to inflammatory processes from both tumor burden and treatments that activate pro-inflammatory cytokine network
Pharmacotherapy
Psychostimulants: methylphenidate (appetite stimulation at lower doses), amphetamine/dextroamphetamine
Stimulants can bolster depressed patient in period before antidepressant takes effect
Combat sedating effects of narcotics
Wakefulness promoting agents: modafinil (low abuse potential, marketed as gentler and less likely than other stimulants to trigger insomnia)
In a randomized placebo-controlled trial, Armodafinil did not improve cancer-related fatigue or change the efficacy of CBT (Heckler et al, 2016)
Antidepressants: unclear if beneficial for patients w/ cancer-related fatigue in absence of depressive mood d/o
Non-pharmacotherapy:
NCCN practice guidelines: self-monitoring of fatigue levels, energy-conserving strategies such as setting priorities, structuring daily routine, attending to one activity at at time, limiting naps to < 1 hr
Exercise: meta-analysis of randomized control trials with moderate effect size (0.34). American College of Sports Medicine recommends cancer patients and survivors do at least 150 min moderate-intensity exercise/week
Insomnia: important to understand etiologies of sleep disturbance for more targeted treatment approach in long-term; in older adults, sleep disturbances can exacerbate certain illnesses and usually don’t improve on their own, so it’s especially important to treat in these patients
Pharmacologic: prescription sleep aids, OTC, herbal supplements; safety and efficacy of sleep medications not yet established in cancer patients!
Recommended sequence of medication trial: 1) short-intermediate acting benzo or ramelteon, 2) alternate short-intermediate acting benzo or ramelteon 3) sedating antidepressant (especially in conjunction with treating depression - trazodone, amitriptyline, doxepin, mirtazapine), 4) combined benzo/ramelteon + sedating antidepressant, 5) other sedating agents (gabapentin, olanzapine)
Zolpidem can be used in short-term
Eszopiclone and Zaleplon have T1/2 of 1 hour = good for patients w/ sleep initiation difficulties
Mirtazapine, nortriptyline, trazodone
Olanzapine and quetiapine in substance users; APDs also preferred over hypnotics in delirium so as not to exacerbate underlying encephalopathy
2/2 depression/anxiety = antidepressant
2/2 steroids = reduction/cessation
2/2 menopausal symptoms = effexor, gabapentin
2/2 OSA = PEEP
2/2 restless leg syndrome = gabapentin, ropinirole, pramipexole
2/2 pain = analgesia
Non-pharmacologic: behavioral therapy, CBT for insomnia (CBTi; best evidence), education, light therapy, exercise, mindfulness, & yoga.
Nausea and vomiting: 2 of the most-feared symptoms among patients with cancer. Antiemetics are better at treating vomiting than nausea.
Chemo-induced nausea and vomiting caused by release of free radicals that cause exocytic release of 5-HT from enterochromaffin cells in gut. Chemo also acts directly on vomiting center via 5-HT3 and NK-1 receptors
High emetogenicity chemos: cisplatin, mechlorethamine streptozotocin, Procarbazine PO, Anthracycline and cyclophosphamide, carmustine, dacarbazine, dactinomycin
Opioids-induced N/V
Intestinal obstruction 2/2 tumor progression, adhesions, post-radiation fibrosis
Radiation-induced N/V - worst with total body irradiation, also moderate risk with upper abdomen irradiation
CNS-related N/V - increased ICP → meningeal irritation which activates mechanoreceptors that stimulate vomiting center
Pharmacotherapy
D2 antagonists: metoclopramide for constipation, early satiety; haloperidol for anxious, agitated, confused
5-HT3 antagonists (5-HT3R has highest frequency in gut and nucleus solitarius): ondansetron (IV, PO), granisetron (Sancuso) can be given transdermally or IV for patient receiving moderate to high emetogenic chemo
NK receptor antagonists: aprepitant, fosaprepitant (water-soluble pro-drug of aprepitant, can be given IV and converted to aprepitant). Greatest impact on delayed N/V from chemo
Steroids: dexamethasone, exact mechanism unknown but may decrease 5-HT release, activate glucocorticoid receptor in medulla and increase levels of other antiemetics; tx of choice for N/V 2/2 increased ICP but be careful with side effects
Cannabinoids: agonism of CB-1 receptors; dronabinol, nabilone but causes impaired psychomotor function and psychoactive effects especially in older patients
Scopolamine - anticholinergic, mgmt of vestibular N/V, nausea related to motion
Mirtazapine - sedation and appetite stimulation via histamine blockade
Haloperidol, perphenazine, olanzapine for nausea
Octreotide: somatostatin analog that reduces gastric secretions by inhibiting vasoactive polypeptide activity - decrease in gut fluid volume improves N/V in bowel obstruction
Anorexia-cachexia syndrome: weight loss, anorexia, muscle and fat loss, wasteful increases in energy expenditure; most closely related to inflammation - inflammatory cytokines (IL-1) modulates appetite at hypothalamus and brain stem centers
Overriding approach is general symptom control - one won’t eat if in severe pain, gasping for breath
Appetite agents
Corticosteroids: stimulate appetite and mood 2/2 anti-inflammatory
Progestational drugs: megestrol, medroxyprogesterone improve appetite and body weight (mostly fat). Caution in hypogonadal pt, concerns about impotence, also increases DVT risk
Cannabinoids: likely improves cortical activity related to taste, smell, enjoyment of food. Recent trial in cancer patients was positive and also showed sleep improvement (Brisebois et al, 2011)
Non-pharmacologic: consider multimodal therapy
Psychosocial therapy: patient and caregivers should be educated that it’s okay not to force feed
Efficacy of exercise and nutrition unclear
Pain: 70% of patients experience severe pain in the course of illness. Pain may occur as part of “cluster” of physical and psychological symptoms; is both sensory and emotional experience
Nociceptive pain results from stimulation of intact nociceptors. Somatic pain from cutaneous or deep tissues - “aching, stabbing, throbbing, pressure-like” while visceral pain involves organs - “gnawing, cramping, aching, sharp” and may be referred
Opioids, non-opioid analgesics
Neuropathic pain results from stimulation of damaged nerve tissue - “burning, tingling, stabbing, shooting, electric shock”
Opioids (used more frequently in cancer-related neuropathic pain because cancer pain often of mixed etiology), anticonvulsants (gabapentin, pregabalin), SNRIs, TCAs, topicals (capsaicin, lidocaine)
Pharmacotherapy: WHO analgesic ladder - non-opioid → weak opioid → stronger opioid → interventional techniques (nerve blocks, epidurals, PCs, spinal cord stimulators)
Mild pain (1-3): NSAID, acetaminophen, consider slow-titration of short-acting opioids if no relief
Moderate pain (4-6): give 5-10 mg oral immediate-release morphine with goal of reducing pain by at least 50%. If < 50% reduction, increased dose by 25-50% and reassess in 4 hrs
Severe pain (7-10): rapidly titrate short-acting opioids
Psychotropic adjuvants: TCAs, SNRIs, mirtazapine, bupropion, trazodone, anticonvulsants
Clinical Pearl: Both the use of opiate medications and insufficiently treated pain may increase the risk of hypoactive delirium.
Psychotherapy
Supportive group therapy, CBT - guide patient to sense of control over pain, relaxation, hypnosis, biofeedback, aromatherapy
Effect Sizes of Treatment Modalities
Effect size is the difference between the treatment and control group, expressed in standard deviation units, where an effect size of 1 means that the treatment arm moved 1 standard deviation away from the control group. 0.8 is considered a large effect, 0.5 is a moderate effect, and 0.2 is a small effect.
Exercise
Meta-analysis of 4881 cancer patient found that exercise significantly reduced cancer-related fatigue by mean effect size of 0.32 during cancer tx and 0.38 following cancer tx (Puetz and Herring, 2012)
American College of Sports Medicine recommends cancer patient and survivors do at least 150 min moderate-intensity exercise per week
Psychotherapy
CBT: research suggests that CBT for depression and anxiety is efficacious, but most existing trials have been done conducted with patients without known diagnosis of MDD or GAD. Ultimately, CBT interventions may help reduce depression, anxiety, as well as cancer-specific physical symptoms (fatigue, insomnia; interestingly anxiety/depression are often secondary outcomes!) and improve QOL
Depression – 1) behavioral activation, 2) correcting negative, automatic thoughts, 3) identify and change core beliefs and schemas
In cancer patients: direct tx of distorted cognitions, feelings of helplessness/pessimism about the future. Also CBT identifies, challenges, and attempts to change recurrent negative self-views of worthlessness, inadequacy.
Anxiety – identify specific worries and address overestimating of likelihood of negative events and/or catastrophizing
CBT > medications for GAD, but it’s also compared primarily with benzodiazepines
Acceptance and commitment therapy (ACT): CBT variant that aims to change the function of distressing thoughts at the individual level to teach patients to reduce the influence of these thoughts on behavior and goal achievement (Rost et al, 2012)
Population: 57 women with stage III or IV ovarian cancer → randomized to TAU or ACT
Vs. TAU (treatment as usual - commonly used cognitive and behavioral components): improvement of distress = .89, anxiety = 1.25, depression = 1.69, QOL = 1.35
Both groups showed improvement in mood and QOL, but ACT had significantly greater improvements
Pharmacotherapy (vs. controls)
Pharmacologic trials: 0.26-0.61, psychotherapeutic trials 0.23-0.95; weighted effect size = 0.43 (Hart et al, 2012)
Meds: fluoxetine, paroxetine, desipramine, mianserin
Desipramine: 0.26
Paroxetine: 0.47
Psychosocial interventions (education, relaxation training): 0.46-0.74 (Jacobsen and Jim, 2008)
Modafinil for cancer-related fatigue: pharmaceutical intervention weighted effect size = 0.09, exercise + psychological = 0.26, psychological 0.27, exercise = 0.3 (Mustian et al, 2017)
Psycho-Pharmacology
CYP450 catalyzes Phase I, where oxidation, reduction, and hydrolysis converts inactive compound (prodrug) to active form, or turns non-toxic molecule into a toxic one
Important isoenzymes: CYP1A2, CYP2C9, CYP2C19, CYP2D6, CYP2E1, CYP3A3/4
CYP2D6 and CYP3A3/4 metabolize most psychotropics
Some anti-neoplastic drugs have pro-drugs that require activation to active metabolites by CYP, or get converted to metabolites with significant toxicity, thus interaction effects crucial
In oncology patients, psychotropic medications are added to complex regimen of chemotherapy agents, antibiotics, analgesics, antacids, antiemetics, steroids, anticonvulsants, bronchodilators, cardio drugs, hormone replacement..
Most psychotropic drugs (except lithium) undergo primarily hepatic metabolism
Pharmacokinetics in cancer patients may be impaired due to:
Mucositis - absorption
Edema, lower levels serum-binding proteins - variation in volume of distribution
Renal/hepatic dysfunction - altered excretion
How Common Are Drug-Drug Interactions?
In cancer patients concurrently receiving antidepressants at MD Anderson Cancer Center in 2006, 49% were found to be taking drug combinations with risk for a major drug interaction with antidepressants (Lal et al, 2011)
40% of patients on antidepressants had major drug interaction that could lead to serotonin syndrome
20% of patients on anticoagulants with risk for major drug interaction
Potential major drug interactions associated with increased number of hospitalizations and ER visits (OR 2.31, CI 1.37-4.03), where patients found to have major drug interaction had 2.5 mean hospitalizations or ER visits, while patients without major drug interaction had 1.6 mean hospitalizations or ER visits (P = 0.01)
Of note, heparin flushes were counted as anticoagulant medications, thus hire rates of hospitalization may be due to patients with higher illness severity requiring IV medications rather than actual drug interactions
Issue of debate: Antidepressants are already underprescribed, as such this article might lead to even more bias and reluctance to treat mood symptoms in cancer patients.

Psychiatric (52%), psychogeriatric (49%), and geriatric (46%) patient populations have high prevalence of patients treated with at least 1 drug metabolized by CYP2D6, with 62% of these classified as antidepressants, followed by antipsychotics as the next most commonly used CYP2D6 substrate (Mulder et al, 2007)
Psychostimulants may inhibit metabolism of anticoagulants, antidepressants, anticonvulsants. They may also antagonize hypotensive effects of antihypertensives while increasing hypertensive effect of pressors (Luigi et al, 2014)
Faster onset of action for terminally ill and cancer patients
May improve attention, concentration, cancer-related fatigue, asthenia
Precautions: cardiac (hypertension), psychiatric (hallucinations, delusions, violent behavior)
Most benzodiazepines are metabolized by CYP450 and have significant potential for interactions. Benzodiazepines metabolized by glucuronidation (lorazepam, oxazepam, temazepam) have fewer drug interactions and are considered 1st line in oncology
In cancer patients concurrently receiving antidepressants and oral anti-cancer drugs at National Cancer Centre Singapore between 2006 and 2009, 21% were found to have potential drug-drug interactions (Chan et al, 2011)
Of 17 pairs of potentially interacting drugs, only 3 were clinically documented to have actually caused interacting effects
CYP2D6 inhibition by fluoxetine leads to reduced efficacy of tamoxifen
CYP2D6 inhibition by fluvoxamine leads to lower plasma concentration of endoxifen
CYP2D6 inhibition by paroxetine leads to reduced efficacy of tamoxifen
There may be potential for electronic drug-drug interaction databases to overcall theoretical drug-drug interactions that may not be clinically significant
Possible solutions include incorporating upper dose limits (drug-drug interactions are typically dose dependent) or identifying patients at risk for adverse events through individual risk assessments
Desvenlafaxine is the major active metabolite of venlafaxine after CYP2D6 metabolism and has low risk of variability when co-administered with CYP2D6 substrates or inhibitors (Low et al, 2018)
Of note, some of the above authors work for Pfizer (manufacturer of desvenlafaxine)
Fluoxetine and paroxetine are strong CYP2D6 inhibitors
Fluvoxamine is strong CYP1A2 and CYP2C19 inhibitor → likely to cause drug-drug interactions
Sertraline, citalopram, escitalopram less likely to cause significant alterations in CYP450, although these can become clinically significant in renally and hepatically impaired patients
Beta-blockers are metabolized by CYP2D6 - antidepressants that inhibit CYP2D6 cause additional HR reduction with given with propranolol, which is both metabolized by and inhibits 2D6 (Bahar et al, 2017)
Clinically significant bradycardia has been reported with paroxetine/fluoxetine and metoprolol
Opioids: fentanyl, methadone, oxycodone are major CYP3A4 substrates, thus inhibitors lead to increased effects
Tramadol undergoes extensive metabolism via CYP2D6 and CYP3A4, but DES doesn’t seem to interfere in major way with CYP-metabolizing pathway of opioids (Pfizer 2016)
+ risk of serotonin syndrome w/ SSRI or SNRI because tramadol has potential SNRI effect
Cancer: pooled prevalence of cancer and comorbid MDD from 31 studies was 10.8% (range 3.7-49%)
Lung cancer: antimicrotubule agents (vinca alkaloids - vincristine, vinblastine, vinorelbine; taxanes - paclitaxel, docetaxel) extensively metabolized by CYP3A4
PK studies showed that Desvenlafaxine is not extensively metabolized by CYP3A4, or does it measurably alter CYP3A4-mediated metabolism (Nichols et al, 2013)
TKIs (erlotinib, gefitinib, osimertinib.. etc) cleared by CYP3A4
Breast cancer: cyclophosphamide, ifosfamide major substrates of CYP3A4 and CYP2B6; doxorubicin is major substrate of CYP3A4 and CYP2D6 → given w/ inhibitors increases concentration and clinical effect of anticancer agents
Colorectal cancer: irinotecan metabolized by CYP3A4 and competitively inhibitors CYP3A4 and CYP2C9
Case report showed potentially fatal rhabdo in patient taking irinotecan and citalopram (CYP3A4 substrate) - speculates theoretical PK interaction between irinotecan and other CYP3A4 substrates such as escitalopram and fluoxetine (Richards et al, 2003)
A Closer Look at Tamoxifen
In a study of 2430 women living in Ontario treated with tamoxifen for breast cancer between 1993 and 2005 w/ overlapping treatment with single SSRI (paroxetine, fluoxetine, sertraline, citalopram, fluvoxamine, venlafaxine), paroxetine use during tamoxifen treatment was associated with increased risk of death from breast cancer. This suggests that paroxetine, a strong irreversible CYP2D6 inhibitor, can reduce the benefit of tamoxifen in women with breast cancer (Kelly et al, 2010)
“absolute increases of 25%, 50%, and 75% in the proportion of time on tamoxifen with overlapping use of paroxetine (an irreversible inhibitor of CYP2D6) were associated with 24%, 54%, and 91% increases in the risk of death from breast
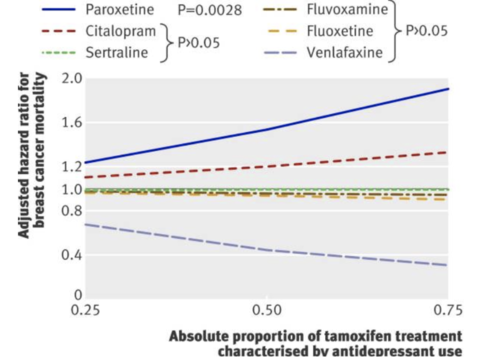
Tamoxifen is metabolized by hepatic CYP450 to active metabolites 4-hydroxytamoxifen and 4-hydroxy-N-desmethyltamoxifen (endoxifen) that have 100x higher affinity for estrogen receptor than parent compound (Jin et al, 2005)
The authors also found a non-significant trend towards reduced breast cancer mortality among venlafaxine users. However, this may reflect the practice of prescribing venlafaxine for hot flashes, which may predict better outcomes in women receiving tamoxifen. Hot flashes are thought to occur when less estrogen is present, and tamoxifene is estrogen receptor blocker (Mortimer et al, 2008)
Paroxetine also associated with increased relative risk of death from any cause; also in subgroup of 226 women w/ unknown cause of death
Interestingly, fluoxetine, a strong CYP2D6 inhibitor, had no association with increased death from breast cancer in this study. Only 10.4% of subjects received fluoxetine while 25.9% received paroxetine.
Clinical Pearl: Strong CYP2D6 inhibitors such as paroxetine and fluoxetine can significantly decrease serum levels of chemotherapy agents, in particular, tamoxifene. Venlafaxine and mirtazapine are weak CYP2D6 inhibitors and may be preferred in patients concurrently receiving chemotherapy.
Interactions between CYP2D6 polymorphisms and coadministered antidepressants that are CYP2D6 inhibitors in women with newly diagnosed breast cancer at Lombardi Comprehensive Cancer Center were found to decrease plasma concentrations of endoxifen, the active metabolite of tamoxifen (Jin et al, 2005)
CYP2D6 homozygous variant or heterozygous had lower plasma endoxifen vs. homozygous WT
Wt/Wt patients using CYP2D6 inhibitors found to have 58% less plasma endoxifen compared to those who did not use CYP2D6 inhibitors
In patients heterozygous for nonfunctional allele, those taking CYP2D6 inhibitors had 38% lower levels of endoxifen
Among those not taking CYP2D6 inhibitor, plasma concentration endoxifen associated w/ CYP2D6 genotype (white bars/triangles represent patients taking CYP2D6 inhibitor)

Plasma endoxifen was slightly reduced in women taking venlafaxine and substantially reduced in women taking paxil

The study found the following inhibition constants for CYP2D6 inhibition: paroxetine (0.05 μmol/L) > fluoxetine (0.17 μmol/L) > sertraline (1.5 μmol/L) > citalopram (7 μmol/L) > venlafaxine (33 μmol/L)
Mental Health and Survivorship/QOL
Depression Care for People with Cancer (DCPC), which consists of pharmacological and psychological collaborative care, is highly effective in improving depression and quality of life in depressed cancer patients, although it does not have significant effect on survival. However, given evidence for improvements to quality of life, treatment of depression is still strongly indicated (Mulick et al, 2018)
SMaRT Oncology-2 trial found that patients with good prognosis cancers who received DCPC had greater treatment response (defined as >50% reduction in Symptom Checklist Depression Scale at 24 weeks); less depression, anxiety, pain, and fatigue; better functioning, health, and quality of life
Secondary analysis of survival outcomes found that 69% of the usual care group and 72% of DCPC group survived to 6 yrs with no significant difference in survival
SMaRT Oncology-3 trial found that patients with lung cancers who received DCPC had significantly lower average depression severity and better self-rated depression improvement, anxiety, quality of life, and role functioning
Secondary analysis of survival outcomes found that 15% of the usual care group and 23% DCPC group survived to 6 yrs
Major depression comorbid w/ cancer affects ~105 patients w/ cancer and associated w/ worse survival in multiple studies (Walker et al, 2014; Satin et al, 2009; Barber et al, 2016; Pinquart et al, 2010)
Previous studies have found that patients on antidepressants prior to breast cancer diagnosis had poorer survival and higher risk of poor quality medical care, suggesting that survival effects of depression may be mediated by quality of medical care
Patients with depression and other mental health conditions receive less population preventive screening for cancer (Mitchell et al, 2014) and diagnosed/treated later (Iglay et al, 2017) → survival disadvantage in patients w/ poor mental health
Depressed cancer patients may be less likely to pursue recommended treatments, have longer hospital stays, higher mortality rates, and higher likelihood of reporting desire for hastened death (Kruse et al, 2015)
Commonly Used Psychotropic Medications




References
Koenig HG, George LK, Peterson BL, Pieper CF. Depression in medically ill hospitalized older adults: prevalence, characteristics, and course of symptoms according to six diagnostic schemes. Am J Psychiatry. 1997 Oct;154(10):1376-83. doi: 10.1176/ajp.154.10.1376.
Mitchell AJ, Chan M, Bhatti H, Halton M, Grassi L, Johansen C, Meader N. Prevalence of depression, anxiety, and adjustment disorder in oncological, haematological, and palliative-care settings: a meta-analysis of 94 interview-based studies. Lancet Oncol. 2011 Feb;12(2):160-74. doi: 10.1016/S1470-2045(11)70002-X. Epub 2011 Jan 19.
Sophie Robinson, David W. Kissane, Joanne Brooker, Susan Burney. A Systematic Review of the Demoralization Syndrome in Individuals With Progressive Disease and Cancer: A Decade of Research. Journal of Pain and Symptom Management. 2015; 49(3): 595-610.
Balaguer A, Monforte-Royo C, Porta-Sales J, Alonso-Babarro A, Altisent R, et al. (2018) Correction: An International Consensus Definition of the Wish to Hasten Death and Its Related Factors. PLOS ONE 13(4): e0196754.
Hermann Faller, Michael Schuler, Matthias Richard, Ulrike Heckl, Joachim Weis, and Roland Küffner. Effects of Psycho-Oncologic Interventions on Emotional Distress and Quality of Life in Adult Patients With Cancer: Systematic Review and Meta-Analysis. Journal of Clinical Oncology. 2013; 31(6): 782-793.
Abbey G, Thompson SB, Hickish T, Heathcote D. A meta-analysis of prevalence rates and moderating factors for cancer-related post-traumatic stress disorder. Psychooncology. 2015 Apr;24(4):371-81. doi: 10.1002/pon.3654.
Jones JM, Olson K, Catton P, Catton CN, Fleshner NE, Krzyzanowska MK, McCready DR, Wong RK, Jiang H, Howell D Cancer-related fatigue and associated disability in post-treatment cancer survivors. J Cancer Surviv. 2016 Feb;10(1):51-61. doi: 10.1007/s11764-015-0450-2.
Heckler CE, Garland SN, Peoples AR, et al. Cognitive behavioral therapy for insomnia, but not armodafinil, improves fatigue in cancer survivors with insomnia: a randomized placebo-controlled trial. Support Care Cancer. 2016;24(5):2059–2066. doi:10.1007/s00520-015-2996-y.
Brisebois TD, de Kock IH, Watanabe SM et al. Delta-9-tetrahydrocannabinol may palliate altered chemosensory perception in cancer patients: results of a randomized, double-blind, placebo-controlled pilot trial. Annals Oncol. 22(9):2086–2093.
Puetz TW, Herring MP. Differential effects of exercise on cancer-related fatigue during and following treatment: a meta-analysis. Am J Prev Med. 2012 Aug;43(2):e1-24. doi: 10.1016/j.amepre.2012.04.027.
Rost, A. D., Wilson, K., Buchanan, E., Hildebrandt, M. J., & Mutch, D. (2012). Improving psychological adjustment among late-stage ovarian cancer patients: Examining the role of avoidance in treatment. Cognitive and Behavioral Practice, 19(4), 508–517. https://doi.org/10.1016/j.cbpra.2012.01.003.
Stacey L. Hart, Michael A. Hoyt, Michael Diefenbach, Derek R. Anderson, Kristin M. Kilbourn, Lynette L. Craft, Jennifer L. Steel, Pim Cuijpers, David C. Mohr, Mark Berendsen, Bonnie Spring, Annette L. Stanton, Meta-Analysis of Efficacy of Interventions for Elevated Depressive Symptoms in Adults Diagnosed With Cancer, JNCI: Journal of the National Cancer Institute, Volume 104, Issue 13, 3 July 2012, Pages 990–1004, https://doi.org/10.1093/jnci/djs256.
Jacobsen, P.B. and Jim, H.S. (2008), Psychosocial Interventions for Anxiety and Depression in Adult Cancer Patients: Achievements and Challenges. CA: A Cancer Journal for Clinicians, 58: 214-230. doi:10.3322/CA.2008.0003.
Mustian KM, Alfano CM, Heckler C, et al. Comparison of Pharmaceutical, Psychological, and Exercise Treatments for Cancer-Related Fatigue: A Meta-analysis. JAMA Oncol. 2017;3(7):961–968. doi:10.1001/jamaoncol.2016.6914.
Lal LS, Zhuang A, Hung F, Feng C, Arbuckle R, Fisch MJ. Evaluation of drug interactions in patients treated with antidepressants at a tertiary care cancer center. Support Care Cancer. 2012 May;20(5):983-9. doi: 10.1007/s00520-011-1170-4. Epub 2011 Apr 26. PubMed PMID: 21519946.
Mulder H, Heerdink ER, van Iersel EE, Wilmink FW, Egberts AC. Prevalence of patients using drugs metabolized by cytochrome P450 2D6 in different populations: a cross-sectional study. Ann Pharmacother. 2007 Mar;41(3):408-13. doi: 10.1345/aph.1H482. Epub 2007 Mar 6. PubMed PMID: 17341534.
Luigi Grassi, Rosangela Caruso, Karen Hammelef, Maria Giulia Nanni & Michelle Riba (2014) Efficacy and safety of pharmacotherapy in cancer-related psychiatric disorders across the trajectory of cancer care: A review, International Review of Psychiatry, 26:1, 44-62, DOI: 10.3109/09540261.2013.842542
Chan A, Yap KY, Koh D, Low XH, Cheung YT. Electronic database to detect drug-drug interactions between antidepressants and oral anticancer drugs from a cancer center in Singapore: implications to clinicians. Pharmacoepidemiol Drug Saf. 2011 Sep;20(9):939-47. doi: 10.1002/pds.2167. Epub 2011 Jul 5. PubMed PMID: 21732473.
Low Y, Setia S, Lima G. Drug-drug interactions involving antidepressants: focus on desvenlafaxine. Neuropsychiatr Dis Treat. 2018;14:567–580. Published 2018 Feb 19. doi:10.2147/NDT.S157708.
Bahar MA, Hak E, Bos JHJ, Borgsteede SD, Wilffert B. The burden and management of cytochrome P450 2D6 (CYP2D6)-mediated drug-drug interaction (DDI): co-medication of metoprolol and paroxetine or fluoxetine in the elderly. Pharmacoepidemiol Drug Saf. 2017 Jul;26(7):752-765. doi: 10.1002/pds.4200.
Nichols A, Liang Y, Matschke K, et al. An evaluation of the potential of cytochrome P450 3A4-mediated drug-drug interactions with desvenlafaxine use. J Bioequiv Availab 2013, 5:1. DOI: 10.4172/jbb.1000134.
Richards S, Umbreit JN, Fanucchi MP, Giblin J, Khuri F. Selective serotonin reuptake inhibitor-induced rhabdomyolysis associated with irinotecan. South Med J. 2003 Oct;96(10):1031-3.
Kelly CM, Juurlink DN, Gomes T, Duong-Hua M, Pritchard KI, Austin PC, Paszat LF. Selective serotonin reuptake inhibitors and breast cancer mortality in women receiving tamoxifen: a population based cohort study. BMJ. 2010 Feb 8;340:c693. doi: 10.1136/bmj.c693. PubMed PMID: 20142325; PubMed Central PMCID: PMC2817754.
Jin Y, Desta Z, Stearns V, Ward B, Ho H, Lee KH, Skaar T, Storniolo AM, Li L, Araba A, Blanchard R, Nguyen A, Ullmer L, Hayden J, Lemler S, Weinshilboum RM, Rae JM, Hayes DF, Flockhart DA. CYP2D6 genotype, antidepressant use, and tamoxifen metabolism during adjuvant breast cancer treatment. J Natl Cancer Inst. 2005 Jan 5;97(1):30-9.
Mortimer JE, Flatt SW, Parker BA, et al. Tamoxifen, hot flashes and recurrence in breast cancer. Breast Cancer Res Treat. 2008;108(3):421–426. doi:10.1007/s10549-007-9612-x.
Mulick A, Walker J, Puntis S, et al. Does depression treatment improve the survival of depressed patients with cancer? A long-term follow-up of participants in the SMaRT Oncology-2 and 3 trials. Lancet Psychiatry, 2018;5:321-6. doi:10.1016/S2215-0366(18)30061-0 pmid:29544711.
J Walker, C Holm Hansen, P Martin, et al. Prevalence, associations, and adequacy of treatment of major depression in patients with cancer: a cross-sectional analysis of routinely collected clinical data. Lancet Psychiatry, 1 (2014), pp. 343-350.
JR Satin, W Linden, MJ Phillips. Depression as a predictor of disease progression and mortality in cancer patients: a meta-analysis. Cancer, 115 (2009), pp. 5349-5361.
B Barber, J Dergousoff, L Slater, et al. Depression and survival in patients with head and neck cancer: a systematic review. JAMA Otolaryngol Head Neck Surg, 142 (2016), pp. 284-288
M Pinquart, PR Duberstein. Depression and cancer mortality: a meta-analysis. Psycholog Med, 40 (2010), pp. 1797-1810.
Pinquart M, Duberstein PR. Depression and cancer mortality: a meta-analysis. Psychol Med. 2010 Nov;40(11):1797-810. doi: 10.1017/S0033291709992285.
Mitchell AJ, Pereira IE, Yadegarfar M, Pepereke S, Mugadza V, Stubbs B. Breast cancer screening in women with mental illness: comparative meta-analysis of mammography uptake. Br J Psychiatry. 2014; 205: 428-435).
Iglay K, Santorelli ML, Hirshfield KM, Williams JM, Rhoads GG, Lin Y3, Demissie K1. Diagnosis and treatment delays among elderly breast cancer patients with pre-existing mental illness. Breast Cancer Res Treat. 2017; 166: 267-275.
Kruse, JL and TB Strouse. Sick and Tired: Mood, Fatigue, and Inflammation in Cancer. Curr Psychiatry Rep (2015) 17:16. DOI 10.1007/s11920-015-0555-3.